
Hepatorenal Syndrome Risk Estimator
Hepatorenal Syndrome Risk Calculator
This tool estimates the risk of hepatorenal syndrome (HRS) based on key clinical parameters. Enter the values from the patient's lab results to assess their kidney function status.
Risk Assessment Results
Key Takeaways
- Liver failure can trigger serious kidney problems, especially hepatorenal syndrome.
- Fluid overload, electrolyte shifts, and increased abdominal pressure all strain the bladder and ureters.
- Early lab monitoring (creatinine, BUN, sodium) and careful diuretic use can slow progression.
- Advanced cases may need renal replacement therapy or liver transplantation.
- Regular follow‑up with both hepatology and urology specialists improves outcomes.
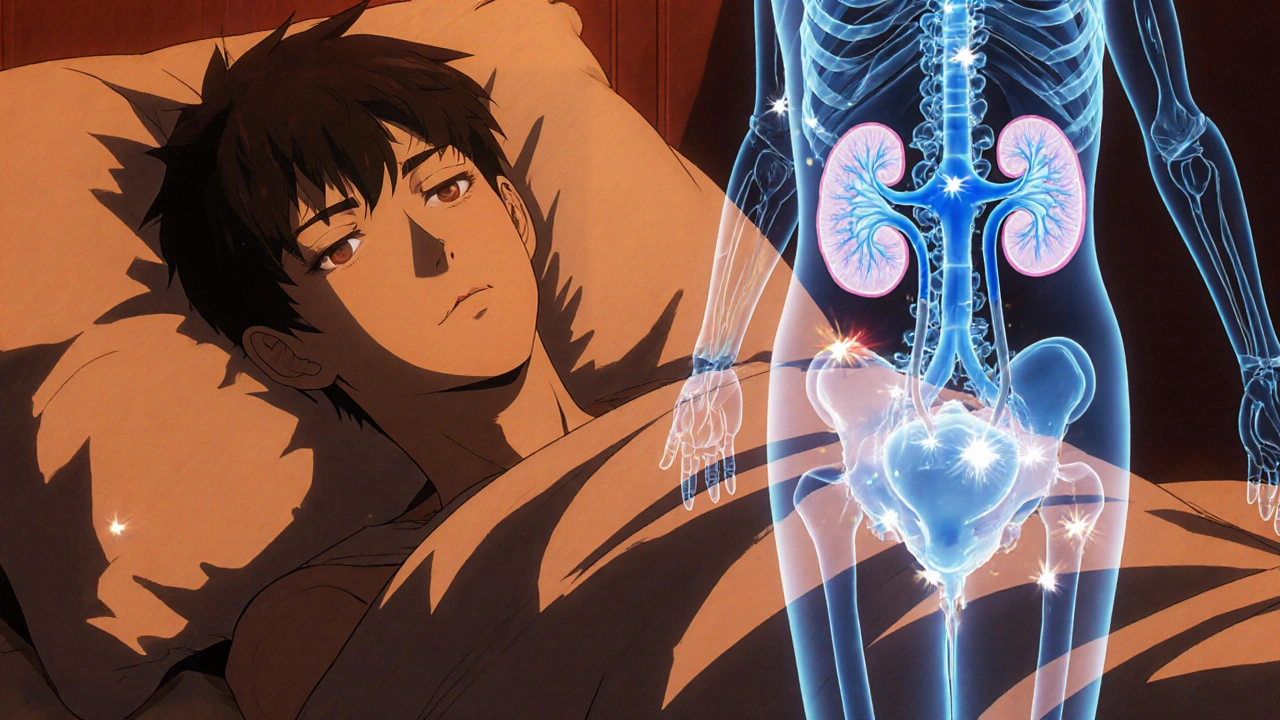
When the liver starts to shut down, the impact ripples far beyond the organ itself. One of the most overlooked downstream effects is on the Urinary system the network of kidneys, ureters, bladder and urethra that filters and excretes waste. Understanding how liver failure a condition where the liver can no longer perform its metabolic, synthetic, and detoxifying functions disrupts this network is crucial for clinicians and patients alike.
What Is Liver Failure?
Liver failure comes in two flavors: acute (sudden loss of function, often from poisoning or viral hepatitis) and chronic (gradual decline, typically due to cirrhosis). Regardless of type, the failing liver can’t produce enough albumin, regulate blood pressure, or clear toxins like ammonia. These deficits set off a cascade that directly compromises kidney perfusion and bladder dynamics.
Why the Urinary System Takes a Hit
The liver and kidneys share a tight physiological partnership. Several mechanisms explain the cross‑talk:
- Reduced effective circulating volume: Low albumin drops oncotic pressure, leading to fluid seeping into the abdomen (ascites). The body reacts by constricting the renal arteries, cutting blood flow.
- Portal hypertension: Elevated pressure in the portal vein pushes blood through collateral pathways, creating a hyperdynamic circulation that further strains the kidneys.
- Neurohormonal activation: The renin‑angiotensin‑aldosterone system (RAAS) fires up, retaining sodium and water, which overloads the bladder and ureters.
- Accumulation of toxins: Ammonia and other metabolites that the liver normally clears can damage renal tubular cells and irritate the bladder lining.
Common Urinary Complications of Liver Failure
Below are the most frequently observed problems, each with its own clinical fingerprint.
- Hepatorenal syndrome (HRS): A functional kidney failure unique to advanced liver disease. It’s characterized by rapid rise in serum creatinine without structural kidney damage.
- Electrolyte imbalances: Hyponatremia (low sodium) and hypokalemia (low potassium) result from excess water retention and diuretic therapy.
- Ascites‑induced bladder compression: The swollen abdomen presses on the bladder, causing urinary frequency, urgency, and incomplete emptying.
- Urinary tract infections (UTIs): Stagnant urine from reduced bladder contractility creates a breeding ground for bacteria.
- Nephrolithiasis risk: Chronic dehydration and altered calcium handling can encourage kidney stone formation.
Spotting the Red Flags - Symptoms & Lab Clues
Early detection hinges on a blend of patient reports and objective tests.
- Decreased urine output (< 500mL/24h) or sudden oliguria.
- Swelling in legs or abdomen despite diuretic use.
- Confusion or asterixis (flapping tremor) - signals accumulating toxins that also affect kidneys.
- Laboratory trends: rising serum creatinine (>1.5mg/dL), falling urine sodium (<10mmol/L), low serum sodium (<130mmol/L), and elevated BUN/creatinine ratio (>20:1).
Management Strategies - Keeping the Urinary System Functional
Effective care blends liver‑targeted treatments with kidney‑friendly tactics.
- Albumin infusions: Restore oncotic pressure, improve renal perfusion.
- Selective vasoconstrictors (e.g., terlipressin): Counteract splanchnic vasodilation, raising renal blood flow.
- Diuretic titration: Use spironolactone plus furosemide in a 100:40 ratio; monitor sodium and potassium closely.
- Paracentesis with albumin replacement: Drains ascites while preventing circulatory collapse.
- Renal replacement therapy (RRT): Consider early dialysis when HRS progresses or fluid overload threatens breathing.
- Liver transplantation: The definitive cure for HRS; post‑transplant kidney recovery is common.
Comparing Major Kidney Complications in Liver Disease
| Feature | Hepatorenal Syndrome | Pre‑renal AKI | Intrinsic Renal Failure |
|---|---|---|---|
| Primary cause | Severe portal hypertension + systemic vasodilation | Volume depletion (bleeding, over‑diuresis) | Acute tubular necrosis, glomerulonephritis |
| Kidney histology | Structurally normal | Usually normal | Damaged tubular cells |
| Response to fluids | Poor; may worsen ascites | Improves with volume replacement | Limited; may need RRT |
| Serum creatinine trend | Rapid rise, often >2mg/dL | Gradual increase | Variable |
| Prognosis without transplant | Months, high mortality | Weeks to months, better than HRS | Depends on underlying cause |
Prevention & Ongoing Monitoring
Staying ahead of trouble requires a regular schedule of checks and lifestyle tweaks.
- Weekly serum electrolytes and creatinine for any decompensated cirrhosis patient.
- Daily weight tracking - a gain of >2kg signals fluid overload.
- Limit sodium intake to < 2g per day; avoid excess alcohol.
- Vaccinate against hepatitisA andB to prevent further liver injury.
- Engage a multidisciplinary team: hepatologist, nephrologist, and urologist.
Frequently Asked Questions
Can liver failure cause permanent kidney damage?
Yes. While early hepatorenal syndrome may be reversible with aggressive treatment, prolonged low kidney perfusion can lead to intrinsic damage that doesn’t fully recover even after a liver transplant.
Why does ascites make me need to pee more often?
The fluid accumulation presses on the bladder, reducing its capacity. Even a small amount of urine triggers the urge to void, leading to frequency and urgency.
Is diuretic therapy safe for someone with liver failure?
Diuretics are essential to control ascites, but they must be carefully dosed. Over‑diuresis can precipitate hepatorenal syndrome, so clinicians monitor electrolytes and urine output closely.
What lab values signal the start of hepatorenal syndrome?
A sudden rise in serum creatinine >1.5mg/dL, urine sodium <10mmol/L, low urine output, and no improvement after plasma volume expansion are classic triggers for HRS diagnosis.
Can a kidney transplant replace a failing liver?
No. Kidney transplantation can address renal failure, but the underlying liver disease will continue to jeopardize the new kidney. In most cases, liver transplantation is the definitive solution.



Nis Hansen
October 17, 2025 AT 19:29When the liver ceases its synthetic duties, the cascade of hemodynamic disturbances begins with a marked reduction in plasma oncotic pressure, which in turn drives fluid into the peritoneal cavity, creating ascites. This fluid shift reduces effective arterial blood volume, prompting activation of the renin‑angiotensin‑aldosterone system and sympathetic nervous system. The resulting vasoconstriction preferentially spares the splanchnic circulation while compromising renal perfusion, a hallmark of hepatorenal syndrome. Moreover, portal hypertension forces blood through collateral pathways, producing a hyperdynamic circulatory state that further taxes the kidneys. The accumulation of nitrogenous waste such as ammonia not only impairs neuronal function but also exerts direct tubular toxicity, aggravating renal insufficiency. Electrolyte disturbances, particularly hyponatremia, arise from inappropriate water retention driven by the same neurohormonal cascade. Simultaneously, diuretic therapy-essential for ascites management-must be titrated carefully; over‑diuresis can precipitate abrupt declines in glomerular filtration. Clinicians should therefore monitor serum creatinine, urine sodium, and daily weight trends with a disciplined schedule. Early detection of oliguria (urine output < 500 mL/24 h) can prompt timely interventions such as albumin infusion or vasoconstrictor therapy. In advanced stages, renal replacement modalities may become necessary while the patient awaits liver transplantation. Multidisciplinary collaboration between hepatology, nephrology, and urology services has been shown to improve survival odds and quality of life. Patient education about sodium restriction (< 2 g/day) and avoidance of nephrotoxic agents remains a cornerstone of preventive care. The interplay between intra‑abdominal pressure and bladder compliance also explains the frequent urgency and frequency reported by patients with large volumes of ascites. Regular cystoscopic evaluation is advisable only when urinary symptoms persist despite optimal ascites control, to rule out secondary infection. Ultimately, the natural history of liver failure illustrates how organ systems are inextricably linked, and a holistic therapeutic strategy is essential to mitigate downstream renal complications.
Understanding these mechanisms empowers both provider and patient to anticipate complications before they become irreversible.
Fabian Märkl
October 31, 2025 AT 15:49Great breakdown, thanks! 😊
Bethany Torkelson
November 13, 2025 AT 23:16This article glosses over the brutal reality that many patients never get the aggressive monitoring they need; weeks can slip by before a rise in creatinine is even noticed, and by then irreversible damage is often done. The reliance on “regular follow‑up” is a polite euphemism for a broken system where specialists are overbooked and labs are delayed. If clinicians truly cared, they would implement point‑of‑care creatinine testing and real‑time alerts rather than hoping patients will report decreased urine output. The lack of emphasis on early vasoconstrictor therapy is especially infuriating, given that terlipressin can reverse hepatorenal syndrome in a significant subset of cases. Moreover, the piece fails to discuss the socioeconomic barriers that prevent many from adhering to low‑sodium diets or frequent weight monitoring. In short, the piece is informative but dangerously optimistic about the feasibility of its recommendations.
Barbara Grzegorzewska
November 28, 2025 AT 10:29Honestly, this write‑up reads like a textbook that forgot to take a sip of coffee – it’s overly stiff and missing that human touch. The author could’ve spiced it up with a bit of anecdotal flair, maybe a tale of a patient who survived the odds, instead of just listing bullet points. Also, let’s not pretendi that “regular follow‑up” magically solves everything; we all know the health system is a tangled web of bureaucratic red‑tape. And while we’re at it, the term “hepatorenal syndrome” could be described in a way that doesn’t sound like a Latin incantation. Definately, a more lively narrative would keep readers engaged rather than put them to sleep.
Avril Harrison
December 11, 2025 AT 04:02Interesting read, especially the part about how ascites can literally press on the bladder and make you run to the loo more often. It’s a reminder that the body’s systems are all connected, and fixing one issue can ripple into others. I’ve seen friends juggling diuretics and still struggling with frequent trips – it’s a real quality‑of‑life thing. Keep the info coming, it helps demystify a lot of the jargon we hear around liver disease.
Natala Storczyk
December 21, 2025 AT 14:02Barbara, you completely miss the point!!! The clinical facts are not a playground for poetic licence – they are life‑or‑death data!!! Your carefree misspelling and flamboyant tone trivialize suffering!! We need rigor, not your “coffee‑sipping” metaphors!! The patients deserve precise, actionable guidance, not a whimsical narrative!!
Rohit Sridhar
December 30, 2025 AT 20:16Avril, you nailed it – the inter‑organ communication is truly fascinating. For anyone coping with cirrhosis, tracking daily weight and keeping a simple diary of bathroom trips can be a game‑changer. Pair that with a low‑sodium diet and regular check‑ins, and you give the liver and kidneys a fighting chance. Stay positive and keep sharing insights; it lifts the whole community.
Sarah Hanson
January 11, 2026 AT 10:02While the article provides a comprehensive overview, it would benefit from clearer delineation between functional and structural renal impairment; such distinction guides therapeutic decisions effectively.
kendra mukhia
January 18, 2026 AT 08:42Sarah, your “concise” note reads like a textbook footnote – utterly detached from the human element. Patients don’t care about “delineation” when their bladder is screaming for relief. A more grounded, empathetic approach is needed, otherwise the information falls flat on a clinical ivory tower.
nitish sharma
February 1, 2026 AT 06:02The integration of hepatology, nephrology, and urology in the management algorithm underscores the necessity of a multidisciplinary framework. Evidence suggests that coordinated care pathways reduce morbidity and accelerate transplant eligibility. Institutions should therefore institutionalise joint clinic sessions to streamline assessment and therapeutic interventions.
Nhasala Joshi
February 8, 2026 AT 04:42nitish, while you champion “multidisciplinary frameworks,” you ignore the shadow network of pharmaceutical lobbying that subtly shapes protocol guidelines. The “evidence” you cite often originates from studies funded by entities with vested interests in proprietary vasoconstrictor drugs. This hidden agenda skews practice patterns, leaving patients exposed to pricey, marginally effective therapies 🙄. The true solution lies in open‑source, peer‑reviewed protocols free from corporate strings-only then can we claim genuine patient‑centered care.